
We will discuss the following aspects of tracheal tubes. Please scroll down and start reading.
- functions of endotracheal tubes
- physical construction
- preformed tubes (e.g. RAE tubes)
- paediatric tubes
- reinforced tubes
- laser resistant tubes
- introduction to double-lumen tubes
- bronchial blockers
- micro laryngeal tubes
What are the functions of endotracheal tubes?
An endotracheal tube :
- provides a passage for gases to flow between a patient’s lungs and an anaesthesia breathing system.
- allows one to provide positive pressure ventilation.
- protects the lung from contamination from gastric contents and nasopharyngeal matter such as blood.
It is a commonly used device that is critical for patient safety so it is important that you understand its design and use.
Endotracheal tubes come in various sizes and shapes, but the basic concepts underlying them are the same for all.
A tracheal tube, as the name suggests, is a tube!
Like any tube, it is:
- made out of certain materials
- has a diameter
- has a length
What are tracheal tubes made out of?
Most endotracheal tubes that you will encounter will be made out of plastic (Polyvinyl Chloride, PVC).
These may be visually clear or opaque.
Plastic is not radio-opaque and therefore plastic tubes have a line of radio-opaque material that makes them more visible on a chest X-ray.

Diameter
Endotracheal tubes have an inner diameter and an outer diameter.
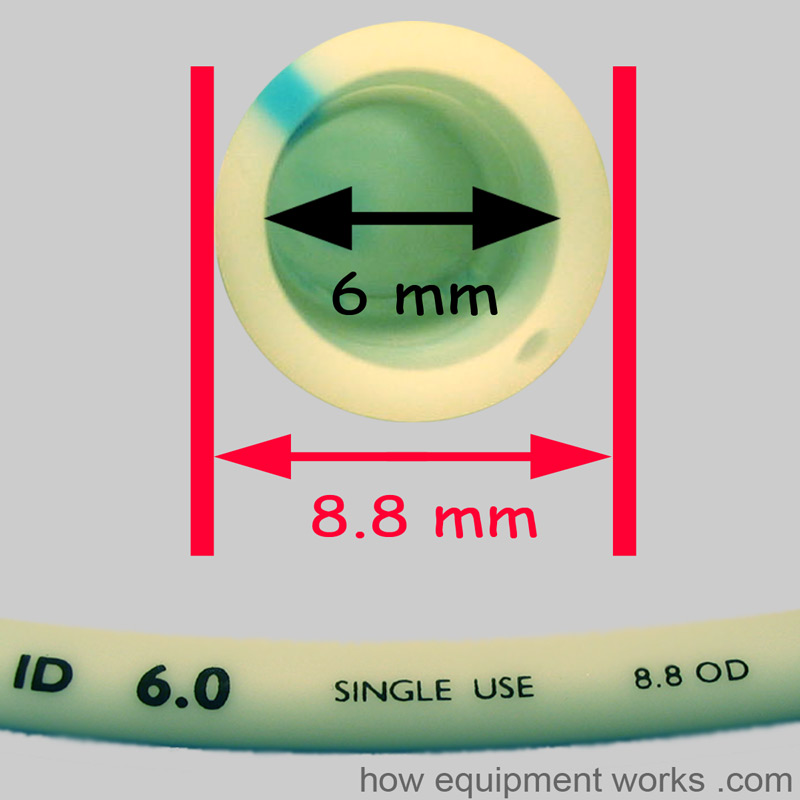
The “size” of an endotracheal tube refers to its internal diameter. Therefore if you ask for a “size 6” endotracheal tube, you are asking for one with an internal diameter of 6 mm. The image below shows a size 6 mm endotracheal tube. In this particular endotracheal tube, the internal diameter is labelled as “ID 6.0” and similarly, the outside diameter is labelled as 8.8 OD.
Narrower tubes increase the resistance to gas flow. A size 4 mm endotracheal tube has sixteen times more resistance to gas flow than a size 8 mm endotracheal tube. This can be especially relevant in the spontaneously breathing patient who will have to work harder to overcome the increased resistance. Thus one should choose the largest diameter endotracheal tube that is suitable for a given patient.
Paediatric endotracheal tubes have a much smaller internal diameter.
Length
The length of an endotracheal tube is measured from the end that goes into the trachea and is marked in centimeters.

After intubation, you should note the “length marking” of the endotracheal tube with reference to a landmark such as incisor teeth or lips. This will help you to monitor the endotracheal tube position and detect if it has moved outwards or further down into a bronchus.
An endotracheal tube that is too long for a given patient may be more prone to kinking and become obstructed. It can be cut to a more appropriate length if necessary.
Below is a photo of probably the longest endotracheal tube in the world! The gentleman is Bob, of Mallard Medical Incorporated, a company that supplies equipment used to anaesthetise large animals. In the image below, he is holding an endotracheal tube used to ventilate elephants. This particular tube has an internal diameter of 45 mm! You can imagine the length of the tube as Bob is six feet (183 centimetres) tall!

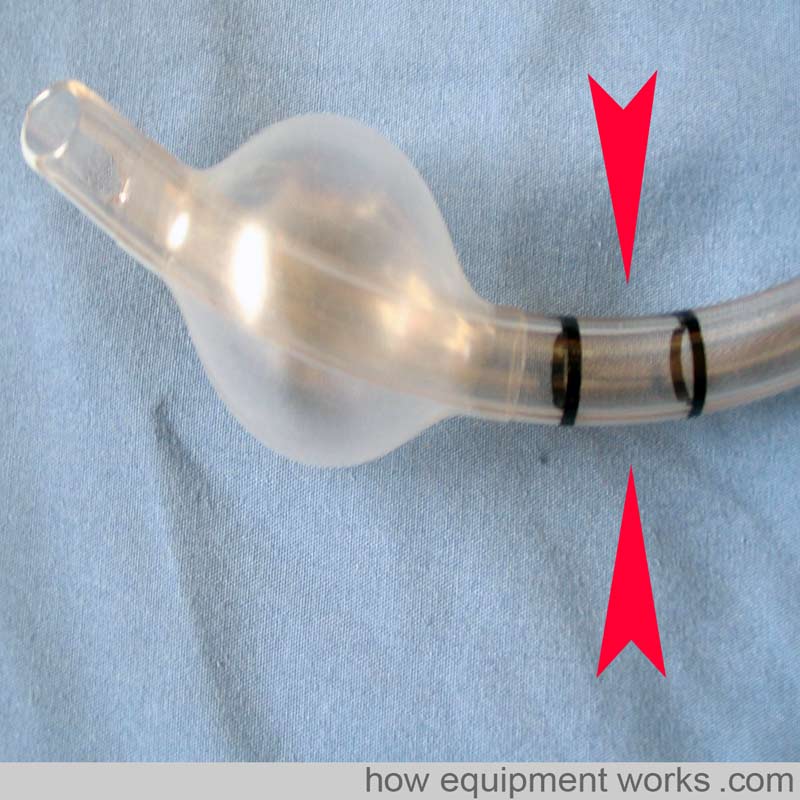
To help with the correct depth of placement, some endotracheal tubes have black markings proximal to the cuff.
As shown below, in endotracheal tubes with only one mark, the vocal cords should be at this mark.
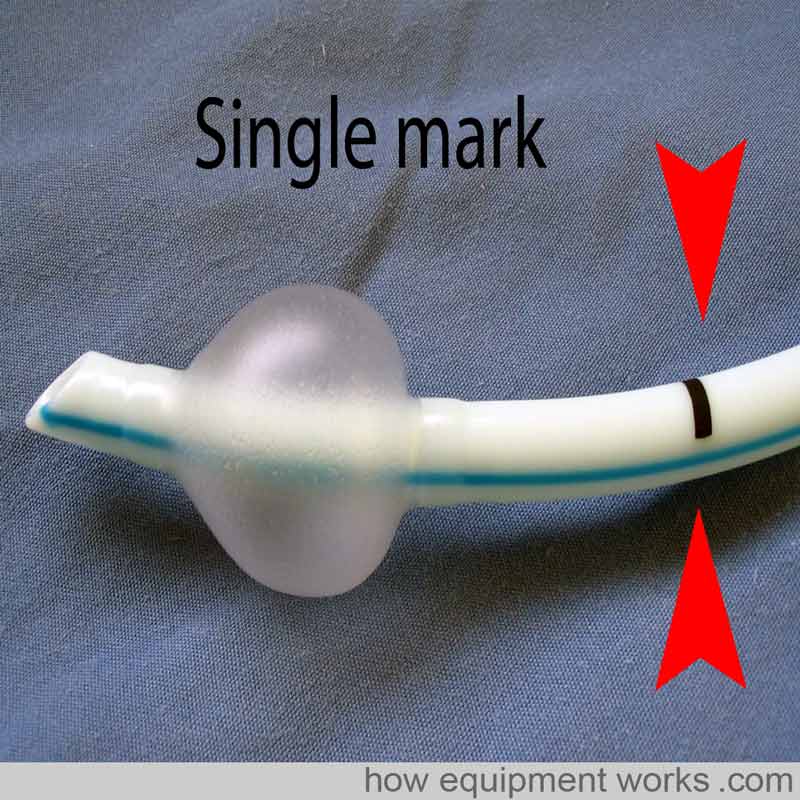
The endotracheal tube shown below has two marks. In this type, keep the vocal cords between the two marks. However, these marking systems only provide a rough estimate and correct endotracheal tube position depth should always be confirmed by auscultation.

Do you work in the anaesthetic team? If you do, please visit the free website below, which has anaesthesia-related fun and safety material. Click the button below to visit.

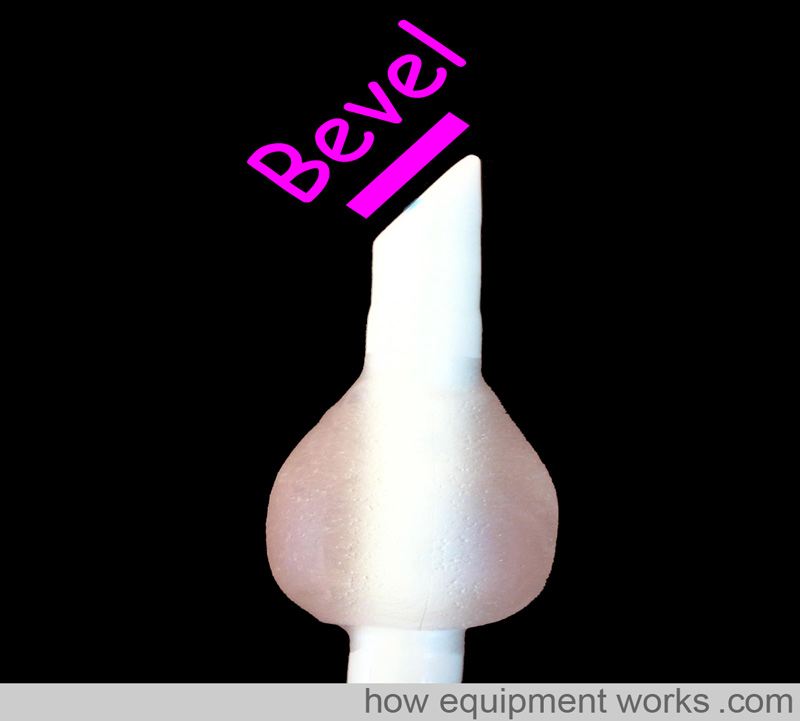
Bevel
To make it easier to pass through the vocal cords and to give you a better vision ahead of the tip, endotracheal tubes have a “slant ” called a bevel.
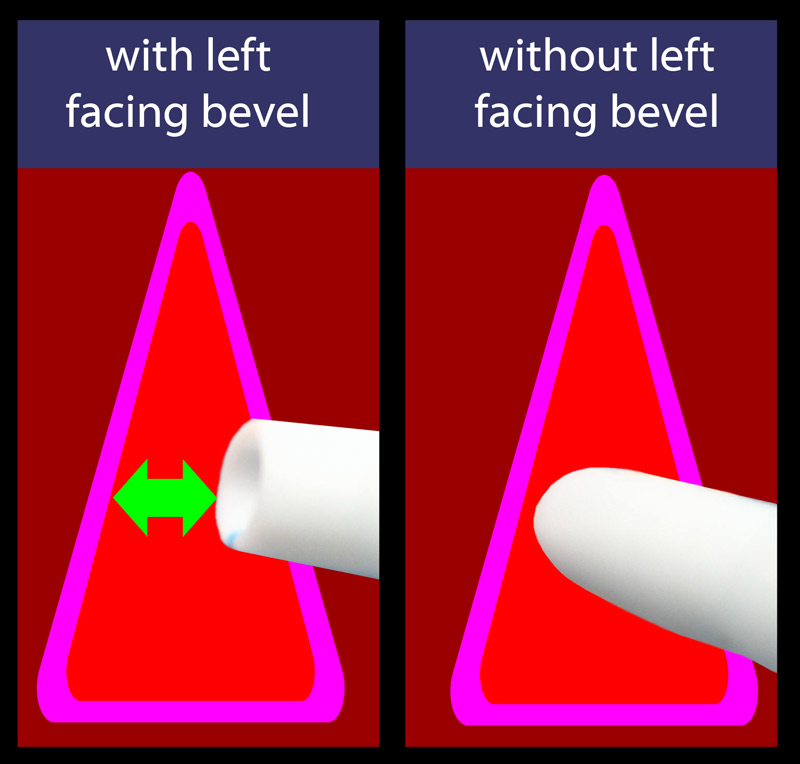
As the endotracheal tube is advanced near the cords, the left-facing bevel gives a better view.
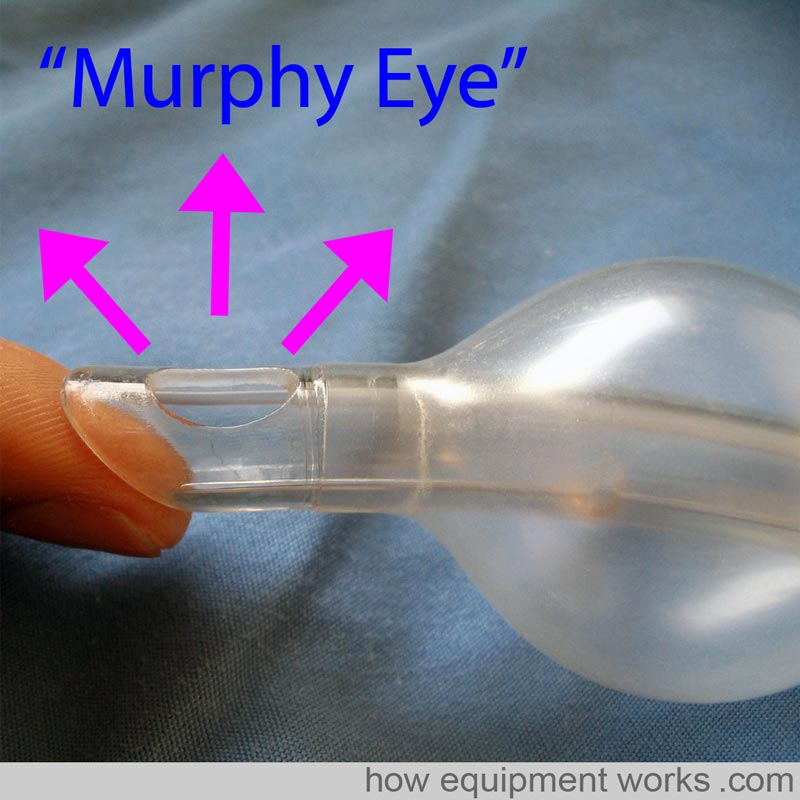
Murphy Eye
Some endotracheal tubes have an additional hole at the tip called a Murphy’s Eye. If the main opening of the endotracheal tube gets blocked by for example abutting against the tracheal wall (represented in the image by my finger) gas flow can still occur via the Murphy Eye. Without the Murphy Eye, the endotracheal tube would have been completely obstructed.
Cuff
A cuff is an inflatable region at the patient end of an endotracheal tube. Endotracheal tubes may or may not have a cuff. In the image below, endotracheal tube 1 does not have a cuff. The endotracheal tube 2 has a cuff that is deflated, and the endotracheal tube 3 has an inflated cuff.
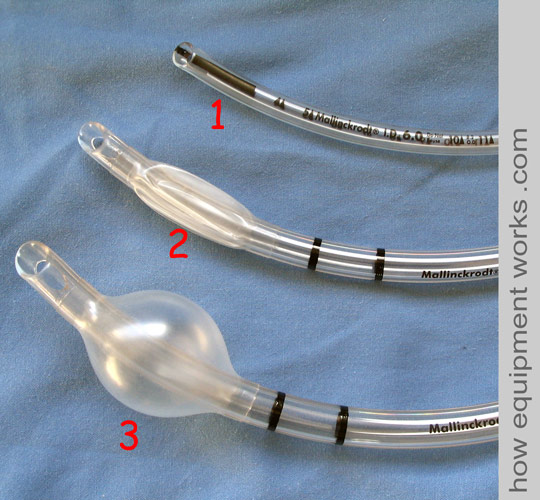
The inflated portion forms a seal against the tracheal wall. This seal prevents gases from leaking past the cuff and allows positive pressure ventilation. The seal also prevents matter such as regurgitated gastric contents going into the trachea.
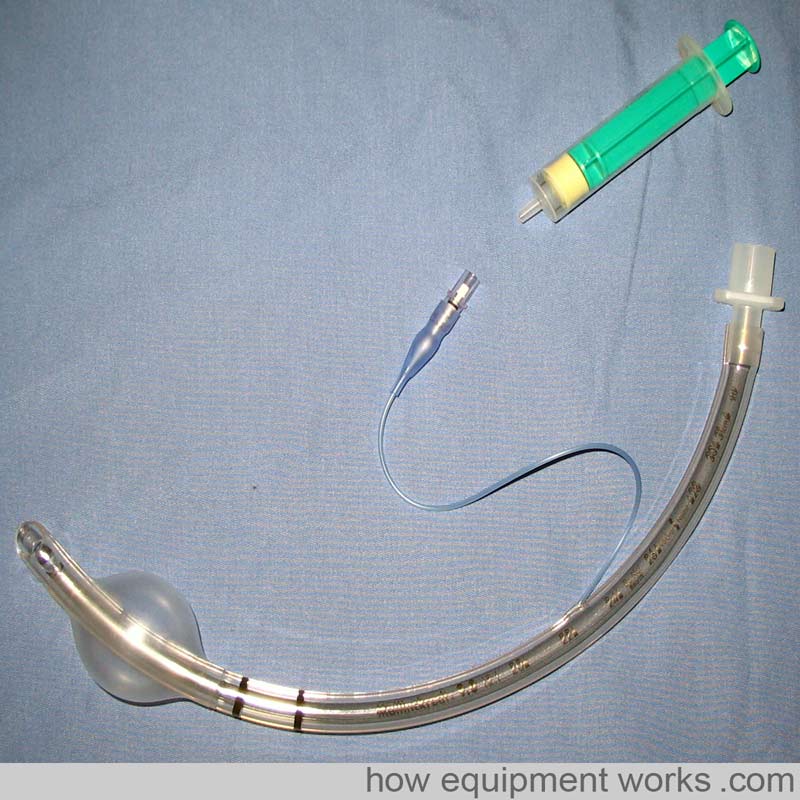
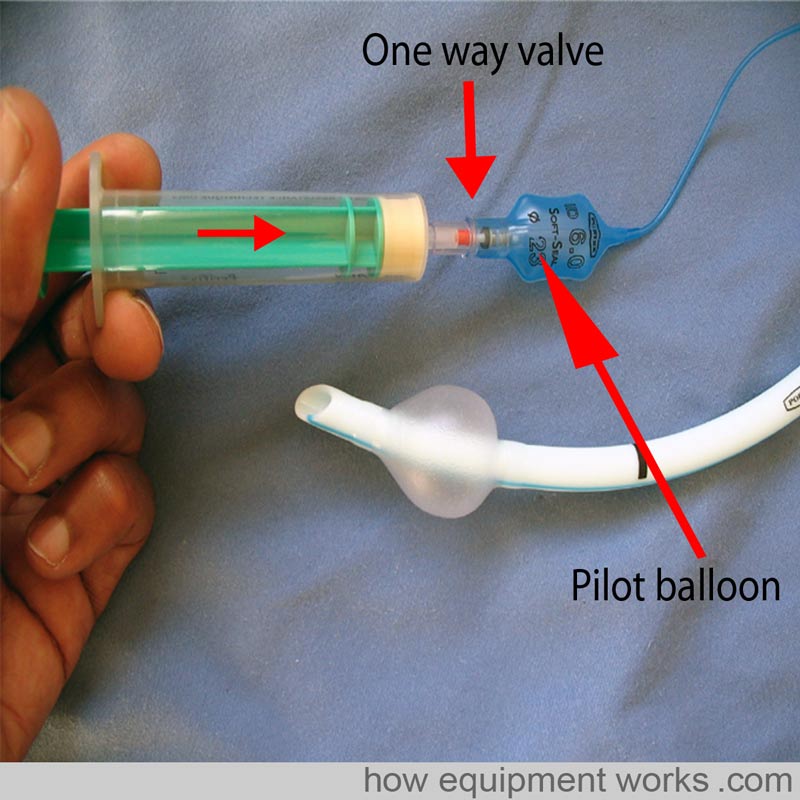
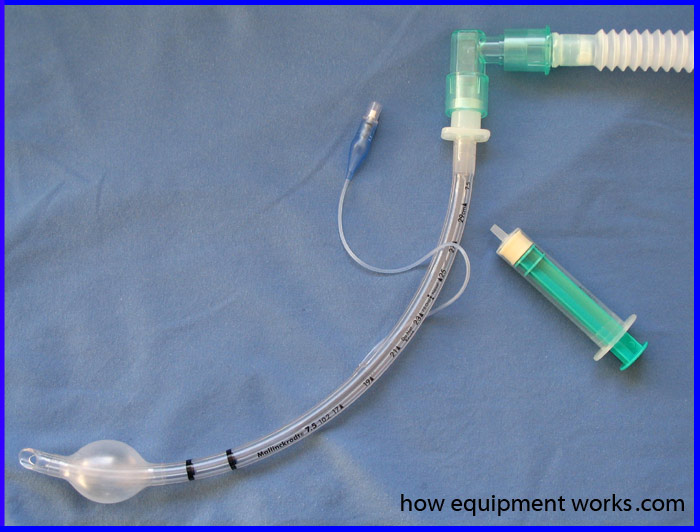
After intubation, the cuff is inflated with air. As shown in the image below, this is done by attaching a syringe to the pilot balloon. A thin tube connects the pilot balloon to the cuff. As the syringe supplies pressurised air, the pilot balloon and cuff inflate. Once the cuff is inflated the syringe is removed. Air does not leak out as there is a one-way valve at the pilot balloon. By feeling the pilot balloon, one can estimate the amount of pressure in the cuff. If the cuff is leaking, e.g. due to damage by the surgeon during a thyroidectomy, the pilot balloon will collapse.
Cuffs are designed to have either a high volume or a low volume.
As explained below, cuffs with a high volume have a low pressure and are called “High volume Low pressure” cuffs. Similarly, cuffs with a low volume have a high pressure and are called “Low volume High pressure” cuffs.
High-volume low-pressure cuffs: As shown in the image below, because of their large volume, they have a larger surface area in contact with the trachea. This means that they apply a lower pressure against the tracheal wall and have a lower incidence of tracheal wall ischemia and necrosis. The seal is not as good as the seal in high-pressure cuffs because of the lower pressures and because the large cuff may develop wrinkles that allow material to pass by the cuff.
Low-volume high-pressure cuffs: These cuffs have a lower volume and the surface area in contact with the trachea is small. This results in a high-pressure seal that is more effective than the one caused by high-volume low-pressure cuffs. However, this high pressure is more likely to cause tracheal ischaemia and necrosis if used for a prolonged period of time.
Connectors
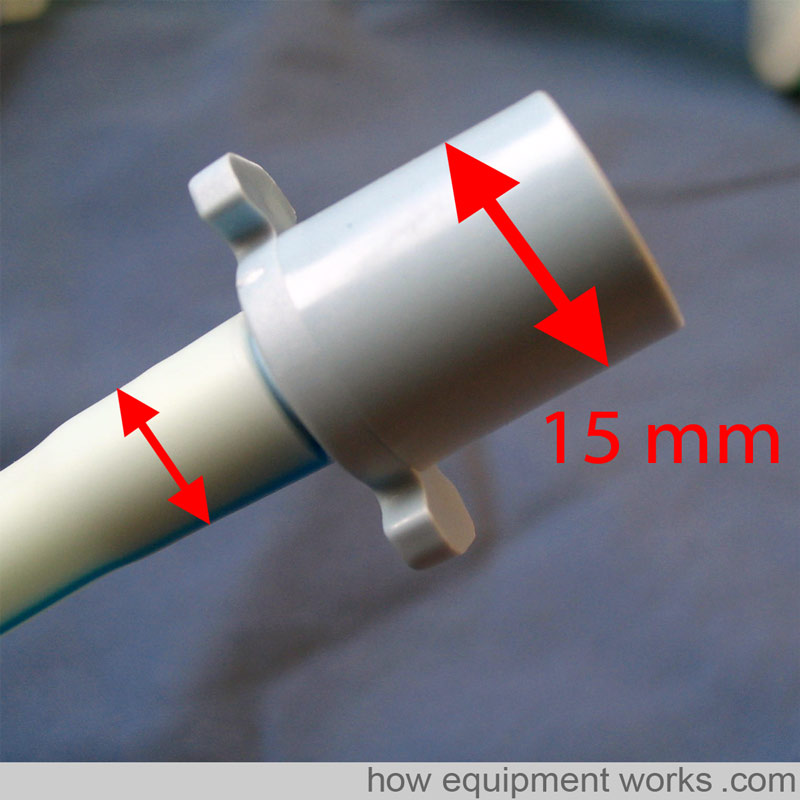
Endotracheal tube connectors connect the endotracheal tube to the breathing system. One end of the connector connects to the endotracheal tube and this end has a diameter that depends on the endotracheal tube size (see small arrows in the image below). The other end connects to the breathing system and has a 15 mm outer diameter (British Standard).
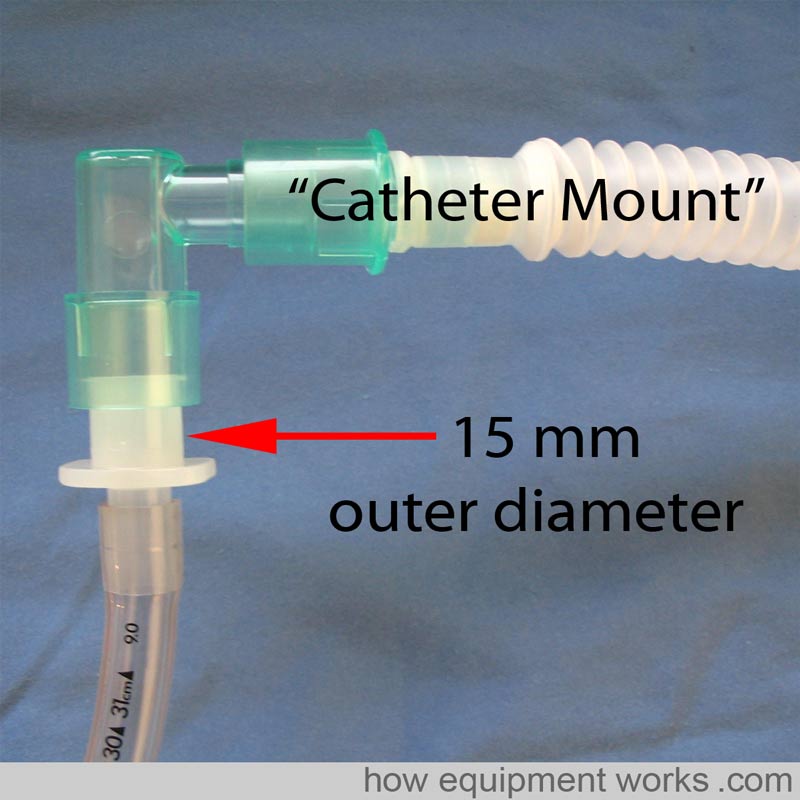
Endotracheal tubes are often not directly connected to breathing systems. Instead, to provide a more flexible connection, endotracheal tubes are often connected to a flexible “Catheter Mount “ (see image below). The catheter mount is then connected to the breathing system.
Special endotracheal tubes
PREFORMED endotracheal tubes
Preformed endotracheal tubes are moulded into special shapes that permit good surgical access in the oro nasal area.
For example (refer to picture below), a “South “ facing preformed endotracheal tube provides good access for the ENT surgeon needing to work in the nasal passages.
Similarly, a “North ” facing (i.e. the tube emerges from the patient and faces towards the patient’s top) preformed endotracheal tube provides very good access to the mouth for dental work.
Below are some pictures of real pre-formed endotracheal Tubes
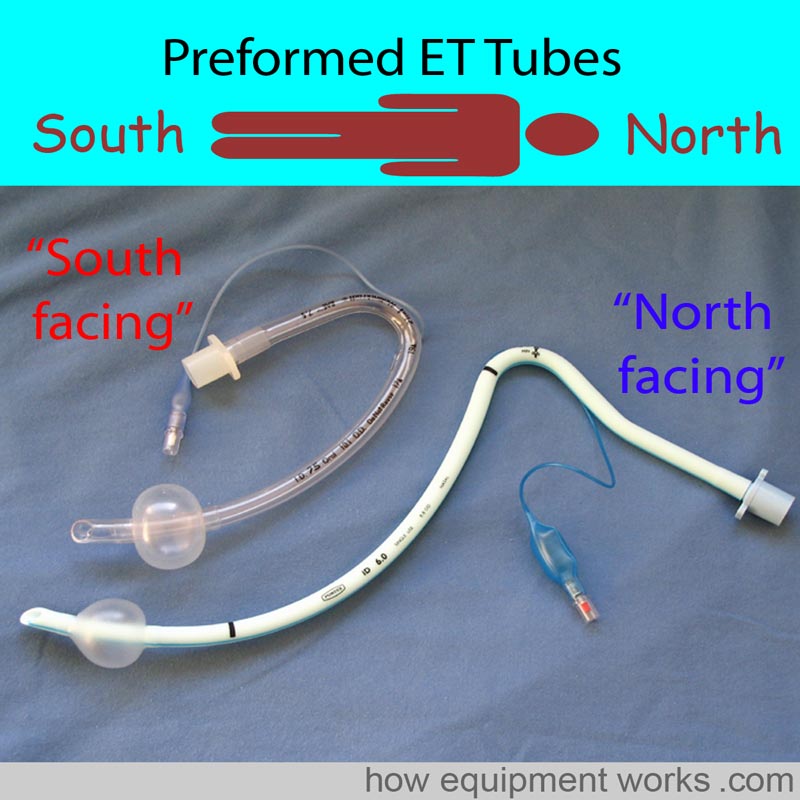
The pre-formed endotracheal below has a special name. It is called a “RAE” tube, named after its inventors Ring, Adair, and Elwyn.

Please click the “Next” button below to read part 2 about tracheal tubes. Thank you.